
By Olena Nitefor, GCFP

Inner Cylinder. Drawing by Suzanne Mertner. Used with permission of the artist.
When it comes to “learning anatomy,” people assume that what they are learning is facts. The joints, the muscles, the nerves… they just are. That is certainly true. But if you think about it, surgeons use their knowledge of anatomy differently from the PT’s who work with the same person post operatively. A Pilates instructor likely utilizes the same factual information differently from a Feldenkrais® Practitioner. I studied anatomy, kinesiology and took a full lab course of cadaver dissection in a Physiotherapy curriculum. We learned joint by joint, studied muscle groups and their actions around joints, and linked joints into joint chains. This was tailored to what was coming ahead: clinical application for working with peoples’ joints and muscles. That is how I started out teaching anatomy in the Feldenkrais® context, because it seemed to me that that WAS the way to teach and to learn. First learn the structures and local functions, and then proceed to global functioning.
In the 30 some years that I have been teaching anatomy in trainings and designing advanced trainings, I have developed a very different approach. I am finding a way of teaching anatomy that is tailored to how we, as practitioners, need to see and understand human movement. Starting with structure and proceeding to function, is not necessarily the best path for us. We need to be able to attend globally, have an understanding of how to sense functional linkages in ourselves, and then look into the skeleton to see how those emerge from the structural possibilities of the joints. This helps us understand the transition from doing ATM® classes to working in FI® sessions. I think we need to start with the skeleton and we need to set its relationships into motion in our thinking, seeing and imagining.
In the Feldenkrais Method® of somatic education we speak about patterns of action, implying that the parts are constellated into action “wholes.” We recall Moshe’s statement that “Someone who thinks in images thinks differently than someone who thinks in words.” Words convey sequential perception, and through words we build an understanding of a whole via an additive process. This plus this plus this. An image, on the other hand, presents a whole in one perceptual schema. We could call these images of “wholes” constellations. The capacity to constellate attention into functional movement relationships between parts of the skeleton is fundamental.
Furthermore, if the brain organizes movement according to intention and image, it needs to plan in images of a whole intended action. It may recruit the components sequentially, but the full image of the movement is preplanned, albeit open for adjustments in relation to sensory feedback. But whatever the movement plan, it must include a support plan!
Therefore, in my approach to teaching anatomy I look for global skeletal relationships of support and focus on understanding the more complex developmental use of the skeleton…turning and walking. From understanding how various parts of the spine contribute to this… and that we are supported by an inner cylinder (the legs do not transmit support in lines upward into the spine.. they transmit support into the pelvic inlet RING…) I fill in the components and elements of the previous developmental stages which are needed to develop towards the final rotational refinement. How does side bending contribute to developing rotation? What is the role of flexion and extension? When are rolling and turning happening simultaneously. When do we substitute rolling for turning and therefore do not develop our capacity for upright support and counter rotation? I weave all this in between ATM experiences. The information lands into experience.
Over the years I have noted that practitioners often observe and think about movement in body part sections: what are the shoulders doing, how is the pelvis turning, where is the head? They then begin to add these together to generate an idea of the whole. Unfortunately, this additive strategy makes it easy to lose the thread of the whole, or to actually miss the fundamental organization of the whole.
Therefore, for years I was hoping to find a bridge into a “constellation of attention” within the skeleton, which unified the action of the whole and was usable in any orientation to space. At least 15 years ago, one such constellation became self-evident to me. It links the trunk and the two significant weight and power transfer regions: the pelvic and shoulder girdles. It includes the spine, is wider/broader than the spine, yet narrower than the outer “cylinder” of the ilia and the ribs. This skeletal “constellation” is the major transfer pathway for gravity and ground forces. Working with it makes it easier to see and strategize within the whole skeleton simultaneously. Practitioners find this ongoingly useful in their personal somatic experience of support as well as for working with clients.
Components of an inner cylinder constellation.
Like any constellation in the sky, this one does not exist. It is a means of organizing attention and gaining clarity about organization. Let’s assemble it.
Pelvic inlet ring:
Because we are bipedal it is very easy to think of weight transfer as following linear paths. Pushing through one leg in Functional Integration®, we think we are finding “the line” of support through the leg into the spine and head. In reality, vertical forces pass through the pelvis via the pelvic inlet ring, and when they arrive there, the forces get distributed into a ring. We are literally supported by a ring of thick, cortical bone, the pelvic inlet.
It’s not this:
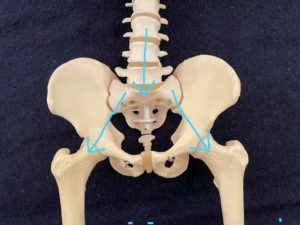
It’s this:
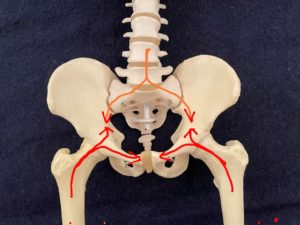
You can read more about this in the article below, from which I have quoted the following sentence:
“The most important force for the pelvic bone, the hip joint force, is predominantly transferred along the superior edge of the acetabulum onto the rest of the pelvic bone towards the sacroiliac joint and the pubic symphysis.” (emphasis mine)
Dalstra, M., & Huiskes, H. W. J. (1995). Load transfer across the pelvic bone. Journal of Biomechanics, 28(6),715-724.
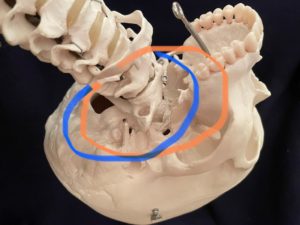
Ring of the first rib:
At the C7/T1 junction we support the head as well as the shoulder girdle and arms. At T1 the first ribs articulate with the vertebra and continue forward, articulating with the sternum behind the sterno-clavicular joint, effectively making a ring at the base of the neck, just below C7. At the time I learned that forces travel into the pelvis in a ring like manner, I realized that the size of the first rib ring was quite similar in diameter to the pelvic inlet ring. Not exact, but sufficient to consider functional implications of linking the two in a constellation for understanding the dynamic between them.
The first rib from above:

In walking, the shoulder and pelvic girdles organize in relation to each other in a contralateral relationship. Proximally, the coordination is organized by the spine, with the two rings, the upper and lower turning in relation to each other. At the best of times, the first rib ring is free to turn in both directions and coordinate with the counter turning in the pelvic ring. The limbs are subsequently organized from the proximal clarity. If the first rib ring is predisposed to turn only one way, the pelvic inlet ring’s turning will be affected. Walking can be disturbed from high in the thorax! The first rib ring and the pelvic inlet ring need to coordinate with each other for a fluid linkage to the limbs.
A quick google search brought me to this website, which considers the ring of the first rib (and individual pairs of ribs below it) and its movement relationship to gait.
How the rings can be constellated into a cylinder.
From the pelvic inlet ring it is easy to descend downward into the small pelvis and imagine a cylinder that emerges via the pelvic floor, with just the ischia making contact when sitting. Upward is a less literal, but very interesting, path on the way up to the first rib. An imagined cylinder would include the sacrum, the spine and the articulations of the ribs with the thoracic segments. It might graze the back of the sternum. Upward the cylinder would include the neck and then reach a further “ring” at the base of the skull behind and on the sides and pass through the TMJ joints, come around to the zygomatic arches, or pass internally behind the upper molars.
Uses of the inner cylinder construct.
When I stand in front of a person and touch the base of their neck with the sides of my little fingers, I immediately have attention within the ring of the first rib and into the inner cylinder. I do not have to think front, back and sides…. The cylinder is an immediate way to have attention within the deep circumference and the volume of the support structures. I have access to all directions, because I have an immediate attentional linkage to the pelvic inlet ring and therefore the legs. I have direct access to how the support system of the legs adapts to the movements from above. I am able to sense how the person’s brain coordinates these two vital areas. I sense the transfer of weight or the turning or the tilt, right where it happens… in the narrowness of the ring, and in the axis of the hip joints which are within the ring. This keeps my movement small and precise and tells me how a person shifts within their base of support. If I go further, I can discover how a person adapts to be taken further out to the edge of their base of support. Staying narrow I find out if they even sense where the highest point of their femurs, and their best support are..
With this inner cylinder in focus we can enter the pathways that gravity and ground reaction forces take through the skeleton from head to foot! That is its value when working with others. When finding this for our clients we will hear that they feel very stable and secure when standing, sitting and walking.
Below are several videos which I made for recent Zoom workshops to explicitly demonstrate the inner cylinder. In teaching, I usually relate anatomy concepts to specific ATMs which we have done. Because the human skeleton repeatedly uses its capabilities for multiple organizations, I simply keep repeating information as it relates to any particular ATM, tag how it is related to the structural possibilities and know that further ATMs will make it possible for the information to be brought forward again. The “language” of anatomy is learned in the context of personal experience, thinking and seeing. It is not a separate study. Occasionally I will bring in muscle images from my preferred anatomy app (Visible Body, Muscle Premium) It allows one to turn the image and see how the musculature attaches from all perspectives. I also value Kapandji’s Physiology of the Joints volumes and several of the books by Blandine Calais-Germain. But the muscular information is always brought in to illuminate experience, not to “learn anatomy” as a subject (or should I say object?)
Anatomy Videos:
Two green discs clearly show the rings. I relate the rotational asymmetries between the two rings to torsion forces into the hips and knees. Watch here.
This video is in relation to AY #407 Heel in the Hand. Watch here.
A pre-pandemic workshop where we look at an aspect of AY #302 Releasing the hips by holding the feet. Watch here.
About Olena:
 Olena Nitefor, M.Ed. graduated in 1987, has assisted in North America and Europe since 1995 and started teaching advanced trainings in the late 90’s. Her background is in modern dance and anatomy. Feldenkrais® Resources released an anatomy video, Sensing and Seeing the Skeleton in the 1990’s (out of print) and Working with the Subjective Middle which is available on the FR site. Her website: https://olenanitefor.com
Olena Nitefor, M.Ed. graduated in 1987, has assisted in North America and Europe since 1995 and started teaching advanced trainings in the late 90’s. Her background is in modern dance and anatomy. Feldenkrais® Resources released an anatomy video, Sensing and Seeing the Skeleton in the 1990’s (out of print) and Working with the Subjective Middle which is available on the FR site. Her website: https://olenanitefor.com